Foundations of Health -- Book Review: Outlive
Book Review of the book Outlive by Peter Attia. One of the best health books in a long time.

Note: this post is unusually long and detailed. You can start with the review and use the detailed section as a reference for healthier living. If you don't get the basics of health and energy right, it will be very hard to have a fulfilling life that achieves your goals.
Peter Attia’s recent book Outlive summarizes much of recent medical knowledge into a comprehensive tome. The core idea is that of “healthspan” as opposed to lifespan. Healthspan is the number of years of healthy, active living that your health provides–one where you’re free to achieve the goals that are meaningful to you.
Attia describes much of the current medical establishment as Medicine 2.0 – with RCTs and short timelines, and an overemphasis on therapeutics. He proposes an idea of Medicine 3.0, where we pay attention to maximizing the healthspan, for which some of the data becomes a bit more predictive and individualized.
In many rich societies, the most likely causes of diminished healthspan come from one of Attia’s “four horsemen:” heart disease, cancer, neurodegenerative disease, or type 2 diabetes along with metabolic dysfunction. The reason these are the diseases of civilization is that medicine 2.0 has become increasingly effective at preventing “fast death” but less effective at “slow death.” Medicine 3.0 is about how to mitigate the risk of diminished healthspan.
An example of Medicine 2.0 is the idea that diabetes is a binary outcome, rather than a continuous phenomena. If your A1c comes in at 6.4%, you’re considered pre-diabetic with a standard set of protocols. If it comes in at 6.5% (glucose 140 mg/dL instead of 137) you’re now considered diabetic with a whole host of different treatment protocols. But in reality, the morbidity is very similar at both levels–and itshouldbe lower than either of those since elevated blood glucose is evidence of metabolic disorder.
Attia’s general prognosis:
Perhaps my biggest takeaway was that modern medicine does not really have a handle on when and how to treat the chronic diseases of aging that will likely kill most of us. This is in part because each of the Horsemen is intricately complex, more of a disease process than an acute illness like a common cold. The surprise is that this is actually good news for us, in a way. Each one of the Horsemen is cumulative, the product of multiple risk factors adding up and compounding over time. Many of these same individual risk factors, it turns out, are relatively easy to reduce or even eliminate. Even better, they share certain features or drivers in common that make them vulnerable to some of the same tactics and behavioral changes we will discuss in this book.
One of those general trends, which has plausible mechanistic links to all of the horsemen: metabolic syndrome. There’s a recent explosion in the number of cases of Non-Alcoholic Fatty Liver Disease (NAFLD) which is an excess of fat that the body doesn’t store well (via viscera). This eventually leads to inflammation which has (probable) pathways to cancer, neurodegenerative diseases and heart disease. There’s a direct pathway to insulin resistance leading to diabetes.
Even if you’re thin, you may have a Metabolic Syndrome and be at elevated risk of the horsemen in your life. Blood work is the best way to tell if you’re at risk – and, there, “normal” readings are not enough. Medicine 3.0 demands that you understand better what the array of markers tell you, and for which ones there is not easy “safe” vs “unsafe” but rather a risk gradient of disease.
Overall this book is incredibly important. Throughout my life the medical “understanding” has been evolving rapidly. I think Attia’s experience as a financial consultant (McKinsey, advising banks) has taught him a unique perspective on relative risk which comes through in this well-informed tome. I highly recommend reading it. Even if not everything ends up being precisely accurate, it makes a very good effort at understanding the phase shift in health and makes it less of a lottery as you age.
Detailed Guide
Read this section for specifics on various dimensions, mirroring the book, podcast interviews, and other resources. If you want a sense of where to start, read the General Framework.
General Framework
The very quick, less narrative summary of the book
- Many major causes of death are “slow deaths” as opposed to “fast deaths” which are traumatic/sudden; you’ll want to reduce all-cause mortality and understand what diminishes health span
- “Slow death” are common things with long lead times, such as the 4 horsemen:
- Atherosclerosis
- Cancer
- Neurodegenerative
- Type-2 Diabetes
- “Slow death” are common things with long lead times, such as the 4 horsemen:
- “Millions of people are suffering from a little-known and underdiagnosed liver condition that is a potential precursor to type 2 diabetes. Yet people at the early stages of this metabolic derangement will often return blood test results in the “normal” range.Unfortunately, in today’s unhealthy society, “normal” or “average” is not the same as “optimal.””
- Exerciseis the most important longevity treatment
- Protein is one of the most important nutrients as you age
- Issue with “medicine 2.0” i.e. current SOTA: Example of HRT (hormone replacement therapy) – there was a 24% increase in breast cancer in the research, offset by a very large amount of benefits. But this risk was an absolute risk of 0.1% (0.4% to 0.5%). Medicine 2.0 would discard; medicine 3.0 thinks about it as an option with risk and reward.
- Concept of Healthspan:
- In order to maximize healthspan, you need to reduce the risks ofallof the horsemen, not just one. As you age, your risk go up –the time to start is early, before youneedit
- Age-related vectors of deterioration: cognitive, physical (muscular strength and fitness are necessary here), and emotional; people often make the mistake of underestimating how much aging drags you down
- Exercise, nutrition and sleep are all very foundational
- Supplements are typically 2nd order in effect compared to the major foundations
- Your individual genotype and risk profile will differ and require different treatments/interventions. Understanding the general risk profile is the important first step.

Goals and Centenarians and Genetics
When thinking about what you should do, here’s a framework to think about:
- When thinking aboutyourold-age objectives, what are they? What is it that you hope to be able to do?
- “Studies of Scandinavian twins have found that genes may be responsible for only about 20 to 30 percent of the overall variation in human lifespan. The catch is that the older you get, the more genes start to matter.”
- The APOE (apolipoprotein E) that is involved in cholesterol transport has 3 variants:
- e2 – much less risk of dementia and correlated to longevity
- e3 – standard combination and baseline
- e4/e4 – 81% less likely to reach old age; up to 12x risk of Alzheimers
- Suggests that cholesterol and lipoproteins matter a lot for long term health
- Rapamycin – works on mTOR – mediator of longevity at cellular level (balance nutrients for growth vs conservation/autophagy) → can be triggered by eating less/fasting
- Limited caloric intake in mice can extend lifespan by 15-45%
- Later studies found that mTOR has 2 complexes, and you only want to suppress 1 for longevity
The Four Horsemen
Insulin and Metabolic Syndrome
Paying attention to your diet, and especially your body’s ability to digest what you are eating is the key principle here. Insulin resistance is the #1 indicator.
- NASH (non-alcoholic steatohepatitis) and its precursor NAFLD (non-alcoholic fatty liver disease) –most patients have no obvious symptoms but would show up with high readings of ALT(alanine aminotransferase) as the first sign something is going wrong in the liver
- Studies suggest that the healthy range is <30 in men and <19 in women, far below the “acceptable” 45 for men and 33 for women. My recent test had this at 75!
- NASH is NAFLD with inflammation, leading to scarring in the liver (this is reversible)
- Metabolic syndrome (MetSyn) is defined as meeting 3 of the following 5 criteria
- Criteria:
- high blood pressure (>130/85)
- high triglycerides (>150 mg/dL)
- low HDL cholesterol (<40 mg/dL in men or <50 mg/dL in women)
- central adiposity (waist circumference >40 inches in men or >35 in women)
- elevated fasting glucose (>110 mg/dL)
- Implications:
- Around 110 mln americans have this, 33mln of which arenot obese– even thin people can be at risk
- Mechanism: as fat overloads your body’s ability to store it subcutaneously it then starts storing in the liver and other visceral organs as well as blood (triglycerides) and muscle (fueling insulin resistance)
- Visceral fat secretes cytokines, driving inflammation near vital organs
- MetSyn is reversible if caught early and mitigated
- DEXA scan can estimate levels of visceral fat (as can the 5 markers)
- Mechanism:insulin resistancemeans that cells have stopped responding to insulin signals (because muscle cells have fat droplets that disrupt glucose channels)
- Eventually you start storing all excess calories as fat
- “Studies have found thatinsulin resistance itself is associated with huge increases in one’s risk of cancer (up to twelvefold), Alzheimer’s disease (fivefold), and death from cardiovascular disease (almost sixfold)—all of which underscores why addressing, and ideally preventing, metabolic dysfunction is a cornerstone of my approach to longevity.”
- Humans are not evolved to do well in consistent abundance (calorically)
- Criteria:
- Fruit smoothies can be badand cause people to fall into MetSyn because the number of calories (and fructose) can actually be too much, too quickly.
- Canary in the coal mine:elevated insulin
Heart Disease
Mental model: no one is “low risk” when you think over the lifespan (yes you might be in the next 10 years, but it’salwaysa healthspan risk).
- Delaying circulatory disease is a key to longevity–and almost none of the damage is actually “sudden”
- HRV (Heart Rate Variability) is a key early health indicator
- Dietary cholesterol has been maligned as a source of blood cholesterol, but most of it is made internally (example of anorexics with high levels of cholesterol, for example)
- Much of the previous research was done in rabbits, where the mechanism is not the same as in humans
- It took nearly two more decades before the advisory committee responsible for the US government dietary guidelines finally conceded (in 2015) that “cholesterol is not a nutrient of concern for overconsumption.”
- (In men) half of all heart attacks occur in under-65s, and a quarter in under-54s; it’snever too early to work on prevention; even at the age of 15 damage could be occurring
- Mechanism: Instead of LDL, thekey underlying factor is apoBas the damaging mechanism, and the goal is lower (and this should be part of your blood test)
- HDL can undo some of the damage with the caveat:
- “But simply raising HDL cholesterol concentrations by brute force, with specialized drugs,has not been shown to reduce cardiovascular risk at all. The key seems to be to increase the functionality of the particles—but as yet we have no way to do that (or measure it).”
- Checking for calcification (later stage) or a ct angiogram (earlier stage soft plaque) are some indicators
- Each standard deviation of apoB increases risk of myocardial infarction by 38%
- Elevated triglycerides can raise apoB
- ⅓-½ of people who consume a lot of saturated fats will see an increase in apoB (goal there is 60% of fats being mono-unsaturated fats–avocados, olive oil, etc)
- Per Attia:you can’t lower apoB too much–every bit lower is better
- If there’s hereditary risk, Attia also checks for Lp(a) levels (the main treatment is lowering apoB)
- Early statins can help manage this risk (especially Crestor, or if tolerance issues, then Nexletol, with some other recommendations at the end of ch7)
Cancer
This is the horseman probably least in your control. But early detect where we have good tests (and evolving quality of liquid biopsies could be a key technology) it makes sense to screen and understand. It also makes sense to control metabolic health all the same.
- Cancer is many types of diseases and pathways and probably the hardest to prevent
- Relatively little is known about the mechanism and causes – so it seems more like luck
- The Cancer Genome Atlas found that some cancer tumors had >100 mutations
- 2 commonalities:
- Very high glucose metabolism (up to 40x the rate of normal cells)
- Unusually good at evading immune system
- Once cancer is established, existing treatments are not as good – catching early is very important
- Link with metabolic dysfunction:
- 12-13% of cases assumed to be attributable to obesity
- Type 2 diabetes can double rates of pancreatic and endometrial cancer
- And BMI >40 increases cancer risk of death by 52% in men, 62% in women
- Attia’s intuition: related to inflammation pathways (and visceral fat)
- Lab animals on caloric restriction had lower rates of cancer (death)
- Anecdote: single survivor of clinical trial had removed added sugar/refined carbohydrates (ketogenic diet) + PI3K inhibitor
- Ketosis can “starve” a cancer, but this is still being studied more
- There is rarely only one way to treat cancer (Mukherjee-Cantlet study) → target multiple vulnerabilities together
- Immunotherapy is a promising field and making progress (success rate is mixed, but resolution is disease free 15+ years later
- Survival rates go up with early detection
- Only good screening for: breast, lung (smokers), prostate, colorectal, cervical\
- Age 40 is probably the right age for first screening (slow-moving disease, earlier incidence over time)
Neurodegenerative Disease
The key idea here is to start early, and while our understanding is still very limited (see Amyloid Hypothesis and its evolution) there are general correlates of brain health, and it makes sense to start investing now, no matter your age.
- The APOE gene has 3 variants, e2/e3/e4
- e2/e2 -20%; e2/e3 -10%; e4/e4 +1100% chance of developing Alzheimers
- APOE plays a role in cholesterol transport and glucose metabolism – and e4 may have defects for this but advantages in resisting disease (promoting inflammation)
- One of the hardest to treat, with limited understanding (and this category includes Lewy body dementia and Parkinsons; less common are ALS and Huntington’s)
- Amyloid (plaque) was thought to be the cause, but treatments of the plaque have not been effective, so people are questioning if that’s a primary driver
- Alternative theory: thatreduced blood flowleads to a “neuronal energy crisis” (e.g. stroke sufferers more likely to be diagnosed with Alzheimers)
- “Vascular disease is not the only culprit here either. In all, some two dozen known risk factors for Alzheimer’s disease also happen to reduce blood flow, including high blood pressure, smoking, head injury, and depression, among others. The circumstantial evidence is strong.”
- Complementary theory: it’s related to glucose metabolism in neurons (and insulin resistance would reduce this)
- Intensive cognitive testing can help distinguish typical aging vs early dementia
- Brains have networks of knowledge (“cognitive reserve”) – the more of these (via language/instruments/etc) the more it seems that people areresistant to cognitive decline
- Similarly, complexmovementlike boxing can delay the progression of parkinsons
- The more complex the intellectual tasks (with nimble thinking/processing) may maintain this cognitive reserve
- Attia’s preventative plan? Mitigate risk by:
- Addressing any metabolic issues (improve glucose metabolism, inflammation, oxidative stress)
- Supplement with omega-3
- Ketogenicmayhelp as ketone metabolism does not decline like glucose metabolism
- Exercise, both cardio and strength training
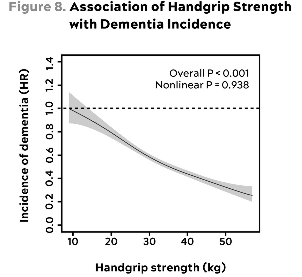
- Grip strength as a proxy for general health and lowest quartile had 72% higher incidence of dementia
- Sleep is a key tool (poor sleep and high stress are multipliers of risk)
- Risk factor: hearing loss (may not be causal, could be correlational and reducing the amount of general brain stimulation)
- Dry saunas have some evidence that it can help too
- Principles:
- Heart health is important for the brain
- liver/pancreas health (metabolic health) is good for the brain
- Start early
- Exercise is the most powerful tool
Tactical Applications
What should you do?
- 5 domains – for optimal health you’ll need to invest in all of these domains
- Exercise
- Nutritional biochemistry (diet)
- Sleep
- Emotional health
- Supplements (exogenous molecules)
- The idea of theCentenarian Decathlon– what 10 (or more) activities are really important for you to do well at the age of 100? Train for those now, while it is much easier to do so. Do much more than that baseline, because all of your health metrics will tend to degrade over time. Attia’s examples include:
- Swim half a mile in twenty minutes.
- Walk with a thirty-pound dumbbell in each hand for one minute.
- Draw back and fire a fifty-pound compound bow.
- Do five pull-ups.
- Climb ninety steps in two minutes (VO2 max = 32).
- Dead-hang for one minute.
- Drive a race car within 5 to 8 percent of the pace I can do so today.
- Hike with a twenty-pound backpack for an hour.
- Carry my own luggage.
- Walk up a steep hill.
- The key point here is that this is a well rounded set of activities
Exercise
Here are the exercise videos on Attia’s site. The exercises are hard to explain in print, so videos are examples to illustrate.
VO2 max– maximum utilization rate of oxygen – may be the most powerful market for longevity
- In the bottom quartile is four times likelier to die than someone in the top quartile
- Going to the next quartile cuts your risk in half
- Attia suggests 5 factors in the study thatsuggestcausality: magnitude, reproducibility, dose-dependence, biologic plausibility and experimental validation (on exercise generally)
- VO2 Max Training?
- 1-2 workouts a week
- ~4-8 minute intervals of the maximum you can sustain, then cooldown/jog for 4 minutes then repeat 4-6x total
- Once VO2 max drops below 18 ml/kg/min in men or 15 in women, people are no longer able to live by themselves easily


Strength(abstract), especially grip strength (reproduced from neurodegenerative section here)
- low muscle mass and low strength were at double risk of death compared to control
- Add in metabolic syndrome and relative risk jumps to 3.3x
- Aging causes degradation in muscle capacity:
- “Longitudinal and cross-sectional studies find that fat-free mass (meaning mostly muscle mass) and activity levels remain relatively consistent as people age from their twenties and thirties into middle age. But both physical activity levels and muscle massdecline steeply after about age sixty-five, and then even more steeply after about seventy-five.”
- Falls are a serious risk to healthspan, if not lifespan, for older folks. Being hospitalized and the corresponding loss in mobility could be permanent.
- Strength and flexibility matter for lowering fall risk
- Older British adults with sarcopenia (muscle loss) were 6x likelier to report low quality of life one decade later
- Bone density also declines with muscle mass, but load bearing activity can offset this (nutrition-protein, heavy load-bearing, HRT, and drugs in order of intended treatment)
- Strength training?
- In general you lose muscle mass much faster than you gain it → being sedentary can be detrimental
- Mental model should be to build up a reserve of strength as a foundation
- Best measure (for health)? How much heavy stuff you can carry
- Attia is a fan of “rucking” – carrying a heavy backpack (60lb) for 1hr on a hike; goal should be to carry ¼-⅓ of your body weight in a pack
- Training regimen:
- Grip Strength
- Concentric and Eccentric load
- Pulling motions
- Hip-hinge movements (e.g. deadlift, step-ups, hip-thrusters, etc) – work your way up to this slowly (e.g. single leg step ups to start)
- Goals / tests you can do:
- Grip strength: ideally males can carry full body weight (½ per hand), females aim for 75% (work your way up to this of course)
- Another one is to just dead-hang from a bar as long as you can (males 2min, females 90s at age 40, with amount going down as you age)
- Eccentric load: step down from an 18 inch block, slowly and smoothly over 3 seconds (note: eccentric strength is a key risk factor as you age, especially for falls)
- Grip strength: ideally males can carry full body weight (½ per hand), females aim for 75% (work your way up to this of course)
- Hip-hinge (see hip hinge)
- Start at 12-inches, body weight to get mechanics
- Attia’s always does first set at 12 inches/body weight
- Get load through center of food (not back) - push down (hamstring engaged); as you load, make sure the femur pushes back
- Your body will try to offset this, keep form good
- Work on eccentric (lowering) control– if it’s hard, you can reach forward to help; do not go up quickly
- 2 ways to increase load: height or additional weight

Stability: maybe the most under-appreciated dimension of physical health (and one related to falls)
- Injury (and subsequently being sedentary) is an enormous factor in age-related decline; stability is one of the best defenses against that
- Mental model: even things like ACL tears are rarely sudden – it could’ve been from years of lack of stability in a joint/chronic weakness; how efficiently can force be transmitted through your body
- DNS (dynamic neuromuscular stabilization) is a training framework that can be relevant
- Keep in mind that so many starting points are different
- Stability Training?
- Aim for 2 dedicated 1-hour sessions per week, with a bit more practice on other days
- Breath – proper breath affects spine, neck, rib, even feet
- Want to strengthen diaphragm: ideal inhalation expands ribs (front/side/back) and belly all at the same time, quietly
- Full exhale (then pause 2s) followed by full inhale, 5 breaths; 2-3 sets
- Elevate legs, something under head – don’t want chin to pop to ceiling
- 1) hand on stomach other on chest; see which hand rises first
- If belly first, then interior tilt
- If chest first, then hyperextension
- Ideal: both hands rise at the same time because you want the diaphragm to descend
- See (breathing)
- Feet – literally the foundation of any movement
- Attia’s trainer suggest toe yoga
- Spread all 10 toes on floor, then try lifting/dropping them individually (egh)
- Mental model is that shoes are actually detrimental to some of the proprioception you’re supposed to have developed
- Matters for balance – can test by putting one foot in front of the other and closing your eyes – can you do that for 10 seconds
- Training toe yoga (see toe yoga):
- Tripod always active
- Lift all toes up, spread ~ 5 seconds, relax
- Next: 2-5 up, big toes down (hold 10-15s)
- Last: 2-5 down, big up (don’t open/cross)
- Keep ankles stable
- Attia’s trainer suggest toe yoga
- Spine – major focus of stability training
- Cat-cow sequence (similar to yoga) where you roll/arch your spine very, very slowly → want extension per vertebra
- Segmental-cat-cow (see segmental cat cow):
- If you don’t have segmental control, you end up hinging which overloads
- Go from cat (extreme flexion) to cow (extreme extension)
- Go forward and backwards very slowly; rest of body is not moving
- Filming yourself (or having a buddy help) so you don’t rush anything
- Shoulders – much more flexible than hip, but much weaker
- Hold light weight/resistance bands then keep arms at your side and raise shoulder blades, then squeeze, then drop, then back to start in a “square”
- Scapular Controlled Angular Rotation (see Scap CARs)
- Shoulder blades up to ears
- Then back
- Then down (still in)
- Then forward
- Once mastered go to circles; also reverse
- Next level: same with arms forward (arm move should only be due to shoulder)
- (important for shoulder and lower back health)
- Rec: video table yourself for form
- Next level: closed-chain (in knees/hands pose) which is much harder
- Hand/finger – distributed strength on the hand (and grip) matters a lot
- Strength section has hip-hinge examples
- Eyes-closed-balance (see eyes closed balance)
- 90% of weight in front leg (“credit-card space” under front heel) – around 30-45 seconds
- Next: close eyes
- Hardest: start to turn head like saying no
Zone 2 Cardio: can maintain a conversation but it might be strained
- It can help train mitochondria: the healthier, the more you can metabolize fat (people with metabolic syndrome were unable to metabolize fat) → for high performance athletes, much of their training is in zone 2 as a foundation for general health
- It can also help with cognition
- “How hard are you working? How easy is it to speak? If you’re at the top of zone 2, you should be able to talk but not particularly interested in holding a conversation. If you can’t speak in complete sentences at all, you’re likely into zone 3, which means you’re going too hard, but if you can comfortably converse, you’re likely in zone 1, which is too easy.”
- How much zone 2? 3 hours a week is probably the lower bound you should target (4 45-minute sessions per week, for example)
Nutrition
Nutrition is crazy hard to study – either the effects measure short term things or have low compliance. Also, there is a verylarge amount of individual variance. This means that things that work for a lot of people may not work for you.
- Attia’s framework:
- Are you under or over nourished?
- Are you under or adequately muscled?
- Are you metabolically healthy or not?
- A few basic rules:
- don’t eat too many calories (or too few)
- consume sufficient protein and essential fats
- obtain vitamins and minerals
- avoid pathogens and toxins
- Very little beyond that isknownwith certainty.
- When looking at a study (any study) keep in mind that general health can be a massive confounder for studies. Example in mice studies below:
- “The low-calorie mice were found to live the longest, followed by medium-calorie mice, and the high-calorie mice lived the shortest, on average. This was the expected result that had been well established in many previous studies.”
- But then Allison did something very clever. He looked more closely at the high-calorie group, the mice with no maximum limit on food intake, and analyzed this group separately, as its own nonrandomized epidemiological cohort. Within this group, Allison found that some mice chose to eat more than others—and that these hungrier mice actually lived longer than the high-calorie mice who chose to eat less. This was exactly the opposite of the result found in the larger, more reliable, and more widely repeated randomized trial. There was a simple explanation for this: the mice that were strongest and healthiest had the largest appetites, and thus they ate more. Because they were healthiest to begin with, they also lived the longest.
- Similarly, the effect of “moderate drinking” with health may actually just be this. Alcohol is a toxin and there may be no “healthy” dose.
- The PREDIMED clinical study (of mediterranean diet) found that olive oil and nuts greatly outperformed a generic “low fat” diet
- Attia has a diatribe about SAD (the Standard American Diet), which has high quantity, cheap, calorically rich, palatable and well preserved. That combination isnothealthy.
- Bad ingredients, in high quantity: added sugar, highly refined carbohydrates, processed oils, other dense caloric foods
Three strategies for nutrition to reduce calories:
- Caloric restriction (CR): eat less in total
- Dietary restriction (DR): cut out certain foods
- Any protein restriction here is likely a bad idea
- If you drop carbs but gain saturated fats, your apoB may skyrocket
- Keep in mind everyone’s metabolism differs
- Time restriction (TR): intermittent fasting
- The main mechanism may just be caloric reduction, but you’re at risk of missing the protein target which could cause loss of lean body mass and gaining fat
- Some extreme cases could involve hypocaloric fasting 1 week a month, for example
- CR is the hardest for many but probably the most direct and effective; but if you are over nourished, you will need to apply some strategy to reduce intake; DR is probably the most common; and TR maybe the easiest for many to implement
- One risk is that with TR, you may lose lean muscle mass too, which actually can make you less healthy in the long run
- Fewer calories tends to lengthen lifespan
- From 2 monkey studies (page 314) the takeaway is thatthe quality of the diet may matter as much as the quantity
- Avoiding metabolic dysfunction is important to longevity
- There’s a link between calories and cancer (the CR monkeys have 50% less cancer)
- Quality matters – the SAD is bad
- If quality is already good, maybe only slight calorie reduction is all that’s needed
Major Food Groups
- A note about alcohol: it’s calorically dense, and serves no nutritional or health purpose
- Carbohydrates: using a continuous glucose monitor can tell you about your individual tolerance and what kinds of inputs lead to what kinds of effects on you
- You will want to obtain a more stable glucose curve throughout the day (spikes can be harmful)
- “Overall, I like to keep average glucose at or below 100 mg/dL, with a standard deviation of less than 15 mg/dL.[*5] These are aggressive goals: 100 mg/dL corresponds to an HbA1c of 5.1 percent, which is quite low.”
- Attia has found, using CGM:
- More refined carbs lead to a faster, higher spike
- Rice and oatmeal cause spikes
- Fructose is missing
- Sleep quality matters a ton (as does stress)
- Spinach and broccoli are neutral
- High protein + fat (eggs, etc) have almost no effect but protein shakes do
- Protein: standard recommended daily allowance is not nearly enough (0.8g/kg)
- Plant proteins can be harder to ingest (and has less of some of the essential aminos)
- A typical 180lb person would ideally have 4 6oz servings of fish, chicken, meat per day
- Some amino supplements have found in studies of old people to lower their liver fat and circulating triglycerides
- Fat: 3 types – saturated fatty acids (SFA), polyunsaturated (PUFA), and monounsaturated (MUFA)
- Many folks have 30-40 from MUFA/SFA and the rest from PUFA (but mostly omega-6 > omega-3)
- Literature is limited, but ideal maybe closer to 55% MUFA, 15-20% SFA and boost EPA/DHA (marine omega-3 PUFA)
- In practice: olive oil, avocados and nuts; cut back on butter and lard and corn/soybean/sunflower oil
- Studies are generally limited/lacking, but it seems like MUFA is the best one and PUFA slightly better than SFA
- You will likely need supplements for EPA/DHA
Sleep
Sleep is incredibly important. It’s easy to think that you can get by on less and try to be more efficient, but there are very real tradeoffs and negative health impacts from not sleeping enough.
- “Scary as it can be in some situations, the short-term harm done by a night or three of poor sleep pales in comparison to the damage that we do to ourselves if this situation continues. Kirk Parsley observed this when he was a physician to the SEALs. Outwardly, these men appeared to be prime physical specimens, finely honed by their rigorous training. But when Parsley analyzed their blood tests, he was shocked:many of these young guys had the hormone levels and inflammatory markers of men several decades older than them—“old-man blood,”Parsley called it.”
- Poor sleep can cause many issues for your metabolism
- “No fewer than nine different studies have found that sleep deprivation increases insulin resistance by up to a third.”
- Poor sleep can cause stress levels to spike (glucocorticoids/cortisol)
- Sleep is also related to brain health
- Some studies are linking poor chronic sleep to Alzheimer’s risk
- REM sleep can help process emotional memories (as well as improve performance on memory tests); REM is also linked to recognition of others emotional states
- Deep sleep is related to “waste removal” processes in the brain
- “More research points to the forties and sixties as the decades of life when deep sleep is especially important for the prevention of Alzheimer’s disease. People who have slept less during those decades seem to be at higher risk of developing dementia later on. Thus, good sleep in middle age appears to be especially important for maintaining cognitive health.”
- Toolkit for Sleep - Huberman Lab – excellent resource for how to sleep better
- Darkness is important, and phones are bad for sleeping well; phones and laptops, etc can disrupt sleep tremendously
- You need your room to be cool to sleep
- Zone 2 cardio can help, especially outside of 2-3 to bed (sunlight exposure is even better for this)
- Journaling something on the top of your mind allows it to relax
- Try to avoid eating within 3 hours before bed
- Lock in a wake-up time, even on weekends, as a way of stabilizing your sleep
- Sleep trackers can track HRV (heart rate variability), breaking rate, etc
- Your chronotype determines whether or not you are a “morning person” etc – this may not be related to sleep quality if you have a late chronotype
Emotional Health
This part of the book is more of an anecdote. It matters, and it’s easily overlooked. But it’s an important part of having a tremendous healthspan.
- Longevity (and the deaths of despair) are also thought of as a mental health crises
- Loneliness is a risk factor for early demise
- Latent traumas can affect quality of life and need to be addressed (5 kinds of childhood trauma: abuse/neglect/abandonment/enmeshment(boundary of adult/child)/witnessing tragedy)
- Coping mechanisms: addiction (including to work), codependency, habituated survival strategies (such as rage), attachment disorders
- Male depression resource that worked for Attia:I Don’t Want to Talk About Itby Terrence Real – “90% of male rage is helplessness masquerading as frustration.”
- “At the Bridge, I learned thatchildren don’t respond to a parent’s anger in a logical way.If they see me screaming at a driver who just cut me off, they internalizethat rage as though it were directed to them.”
- Mindfulness can create space between input and feeling – and can break unhealthy habit links
- Sometimes, you can change how you feel by changing how you act. Behavior change can lead to mood change.